
Summary
Background
WHO has called for increased testing in response to the COVID-19 pandemic, but countries have taken different approaches and the effectiveness of alternative strategies is unknown. We aimed to investigate the potential impact of different testing and isolation strategies on transmission of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2).
Methods
We developed a mathematical model of SARS-CoV-2 transmission based on infectiousness and PCR test sensitivity over time since infection. We estimated the reduction in the effective reproduction number (R) achieved by testing and isolating symptomatic individuals, regular screening of high-risk groups irrespective of symptoms, and quarantine of contacts of laboratory-confirmed cases identified through test-and-trace protocols. The expected effectiveness of different testing strategies was defined as the percentage reduction in R. We reviewed data on the performance of antibody tests reported by the Foundation for Innovative New Diagnostics and examined their implications for the use of so-called immunity passports.
Findings
If all individuals with symptoms compatible with COVID-19 self-isolated and self-isolation was 100% effective in reducing onwards transmission, self-isolation of symptomatic individuals would result in a reduction in R of 47% (95% uncertainty interval [UI] 32–55). PCR testing to identify SARS-CoV-2 infection soon after symptom onset could reduce the number of individuals needing to self-isolate, but would also reduce the effectiveness of self-isolation (around 10% would be false negatives). Weekly screening of health-care workers and other high-risk groups irrespective of symptoms by use of PCR testing is estimated to reduce their contribution to SARS-CoV-2 transmission by 23% (95% UI 16–40), on top of reductions achieved by self-isolation following symptoms, assuming results are available at 24 h. The effectiveness of test and trace depends strongly on coverage and the timeliness of contact tracing, potentially reducing R by 26% (95% UI 14–35) on top of reductions achieved by self-isolation following symptoms, if 80% of cases and contacts are identified and there is immediate testing following symptom onset and quarantine of contacts within 24 h. Among currently available antibody tests, performance has been highly variable, with specificity around 90% or lower for rapid diagnostic tests and 95–99% for laboratory-based ELISA and chemiluminescent assays.
Interpretation
Molecular testing can play an important role in prevention of SARS-CoV-2 transmission, especially among health-care workers and other high-risk groups, but no single strategy will reduce R below 1 at current levels of population immunity. Immunity passports based on antibody tests or tests for infection face substantial technical, legal, and ethical challenges.
Funding
UK Medical Research Council.
Introduction
Different countries have taken very different approaches to molecular testing in response to the COVID-19 pandemic. The observation that countries with high rates of testing for severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection have effectively controlled transmission (eg, South Korea and Germany) has led to calls for increased testing in other countries with lower rates of testing (eg, the UK and the USA). However, the contribution of testing to COVID-19 control compared with other interventions such as self-isolation and physical distancing is currently unclear.
There is a clear priority to test patients with suspected COVID-19 in hospital to inform treatment and infection control strategies, and to monitor the extent of the pandemic. As testing capacity increases, the role of wider testing in different risk groups should be determined, not only to monitor the pandemic but also to prevent transmission by isolating infected individuals. Targets for testing could include health-care and social-care workers, care home residents, other high-risk groups, or the general population.
- Semple C
- Docherty A
- Green C
- et al.
to 19% in Spain
Informe sobre la situación de COVID-19 en España. Informe COVID-19 no 22.
). This high incidence (six-fold higher than in the general population in the UK
Coronavirus (COVID-19) infection survey pilot.
) reflects their exposure to SARS-CoV-2 infection from patients and fellow staff. Infection in health-care workers can contribute to nosocomial spread of SARS-CoV-2, and similar concerns apply to transmission among care home staff and others working with vulnerable populations. Regular screening of these high-risk groups for infection, in addition to routine testing of those with COVID-19 symptoms, could identify individuals with mild or asymptomatic infection and reduce SARS-CoV-2 transmission if they self-isolate.
Evidence before this study
Evidence on the performance of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) tests has been accumulating, and our understanding of COVID-19 epidemiology has been evolving rapidly, with much of the scientific evidence still only available as preprints rather than peer-reviewed publications. We therefore searched PubMed and the medRxiv preprint server (using the R package medrxivr) using the search term “(SARS or COVID or coronavirus) and test* and model and math*” on June 1, 2020, for papers published or uploaded in 2020. The search returned 20 publications and 43 preprints, from which we identified 11 studies that used mathematical modelling to evaluate the role of testing in COVID-19 control, including two preprints missed by the search but known to the authors. Two studies examined regular screening of health-care workers for infection, one considered the effectiveness of test-and-trace strategies (assuming 100% test sensitivity), three studies examined universal mass testing (irrespective of symptoms), and six modelled increased testing simply as an increase in the rate at which infections were detected and isolated. Model results were often divergent, reflecting different assumptions about SARS-CoV-2 epidemiology and testing capacity. Weekly screening of health-care workers was estimated to prevent between 5% and 24% of transmission from this group, test and trace reduced the reproduction number (R) for SARS-CoV-2 transmission between 15% and 50% depending on coverage and timeliness of test results, and estimates for the effectiveness of universal mass testing varied, from a 2% reduction in R to a 40% reduction in epidemic size, depending on coverage and frequency. Very few studies considered test performance (sensitivity and specificity) and only one study considered more than one testing strategy.
Added value of this study
Our study evaluates the optimal use of available SARS-CoV-2 nucleic acid and antibody tests for prevention of transmission. We developed a mathematical framework describing infectiousness and test sensitivity over time since infection to estimate the effectiveness of alternative strategies, including regular screening of high-risk groups such as health-care and social-care workers and the effectiveness and efficiency of test-and-trace protocols. We integrated current evidence for the sensitivity and specificity of available tests alongside epidemiological data about the proportion of asymptomatic infections and the contribution of individuals with asymptomatic and presymptomatic infections to transmission. We did sensitivity analyses to determine the robustness of our results and considered the implications of our findings for national testing policies.
Implications of all the available evidence
Testing can play an important role in the prevention of SARS-CoV-2 transmission, in addition to its established use for pandemic surveillance and confirmation of a COVID-19 diagnosis. Optimal strategies should include regular screening of high-risk groups such as health-care and social-care workers during periods of sustained transmission, and testing of people with COVID-19 symptoms and tracing and quarantining their contacts. Test and trace requires high coverage (proportion of cases tested and contacts successfully traced and quarantined) and rapid testing and contact tracing to be effective. Testing alone is unlikely to bring R below 1 at current levels of immunity and will need to be complemented by other interventions such as physical distancing.
Testing could also contribute to prevention of SARS-CoV-2 transmission in the general population. It might promote adherence to self-isolation by individuals showing COVID-19 symptoms who test positive. It is also the basis of test-and-trace interventions, which involve tracing and quarantining contacts of laboratory-confirmed cases.
- Evans S
- Agnew E
- Vynnycky E
- Robotham JV
,
- Kretzschmar ME
- Rozhnova G
- Bootsma M
- van Boven ME
- van de Wijgert J
- Bonten M
,
- Kucharski AJ
- Klepac P
- Conlan AJK
- et al.
,
However, these studies have assumed 100% accuracy of available tests or that testing simply increases the rate at which infected individuals are isolated.
We aimed to investigate the potential impact on SARS-CoV-2 transmission of alternative strategies for deploying PCR tests that identify active infection and antibody tests that indicate past infection. We developed a mathematical model of transmission to estimate the effectiveness of strategies aimed at health-care workers, other high-risk groups, and the general population, including regular testing irrespective of symptoms and test-and-trace strategies. We also explored the concept of so-called immunity passports, which have been proposed as an approach to certify individuals with evidence of past infection or acquired immunity as safe to return to work where there may be risk of exposure to SARS-CoV-2. We focus on the UK, but our results are relevant for policy decisions made by other countries.
Methods
Mathematical model
We used this model to evaluate the impact of self-isolation following either a positive test result or symptom onset, and the impact of quarantine of contacts of laboratory-confirmed cases. We assumed a proportion of infections are asymptomatic and that individuals who are asymptomatic might have lower infectiousness than those with symptomatic infections. We derived formulae for the effective reproduction number (R), defined as the average number of secondary infections from a single infected individual, in a population with testing of individuals with symptomatic infection only, screening of all individuals irrespective of symptoms, and test and trace, where contacts of laboratory-confirmed cases are quarantined. We calculated the expected effectiveness of different testing strategies, defined as the percentage reduction in R. We did sensitivity analyses of these model estimates to uncertainty in model parameters using bivariate plots and Latin Hypercube Sampling from model parameters with 1000 replicates to generate 95% uncertainty intervals (95% UIs). The model is described in detail in the appendix (pp 2–4) and the full code is online.
Model parameters and data
- Borremans B
- Gamble A
- Prager KC
- et al.
,
- Kucirka LM
- Lauer SA
- Laeyendecker O
- Boon D
- Lessler J
,
- Wikramaratna P
- Paton RS
- Ghafari M
- Lourenco J
Specificity of PCR was assumed to be 100% on the basis of the performance of the majority of available tests reported by the Foundation for Innovative New Diagnostics.
Interactive dashboard of SARS-CoV-2 diagnostic performance data.
We extracted data on the sensitivity and specificity of IgG (or IgG plus either IgM or IgA) antibody tests based on tests of samples from PCR-positive COVID-19 cases in the same Foundation for Innovative New Diagnostics database accessed on June 3, 2020.
Interactive dashboard of SARS-CoV-2 diagnostic performance data.
We used these data to determine the positive predictive value of a positive antibody test that might be used to issue an immunity passport.
Role of the funding source
The sponsor of the study had no role in study design, data collection, data analysis, data interpretation, or writing of the report. The corresponding author had full access to all the data in the study and had final responsibility for the decision to submit for publication.
Results
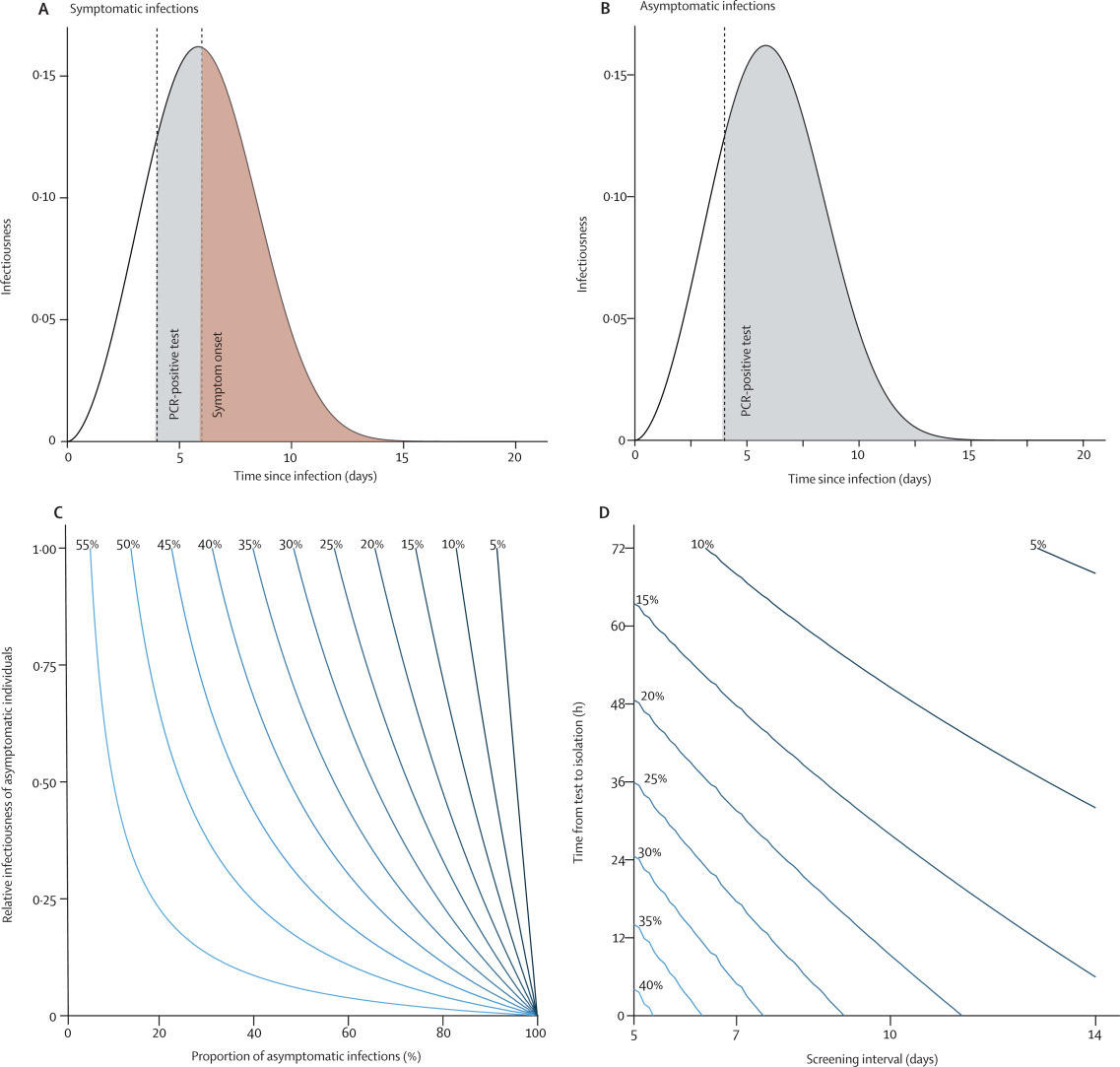
Figure 1Infectiousness of SARS-CoV-2 over time since infection estimated from the serial interval and the reduction of transmission as a result of self-isolation after symptoms or a PCR-positive test result
(A) Detection of presymptomatic SARS-CoV-2 infection and subsequent reduction in transmission through self-isolation after a positive PCR test. (B) Detection of asymptomatic SARS-CoV-2 infection and subsequent reduction in transmission through self-isolation after a positive PCR test. The shaded areas in these plots illustrate infectiousness that would be limited by PCR testing (grey) at 4 days after infection or self-isolation following symptom onset (red) at 6 days after infection. The area under the curves is equal to the reproduction number. (C) Percentage reduction in the reproduction number by self-isolation following onset of symptoms as a function of the proportion of infections that are asymptomatic and their relative infectiousness compared with symptomatic infections. (D) Additional percentage reduction in the reproduction number by a policy of repeated PCR testing at regular intervals with different timeliness from sample collection to isolation, assuming a third of infections are asymptomatic and that they are 50% as infectious as symptomatic infections. SARS-CoV-2=severe acute respiratory syndrome coronavirus 2.
PCR testing of symptomatic individuals to identify SARS-CoV-2 infection would reduce the number of individuals needing to self-isolate. However, it would also reduce the effectiveness of self-isolation because some test results would be false negatives. If samples were collected close to the time of symptom onset and test results were made available rapidly (eg, within 24 h), then the proportion of false-negative results would be relatively low (around 10%) on the basis of the reported PCR test sensitivity, and most symptomatic individuals could safely return to work once well. For example, with a 1% prevalence of SARS-CoV-2 infection, a single negative test would have a greater than 99% probability of being correct (negative predictive value). A negative test would also release any quarantined household members who might be required to stay at home (eg, in the UK, cohabitants of someone with COVID-19 symptoms currently need to quarantine for 14 days).
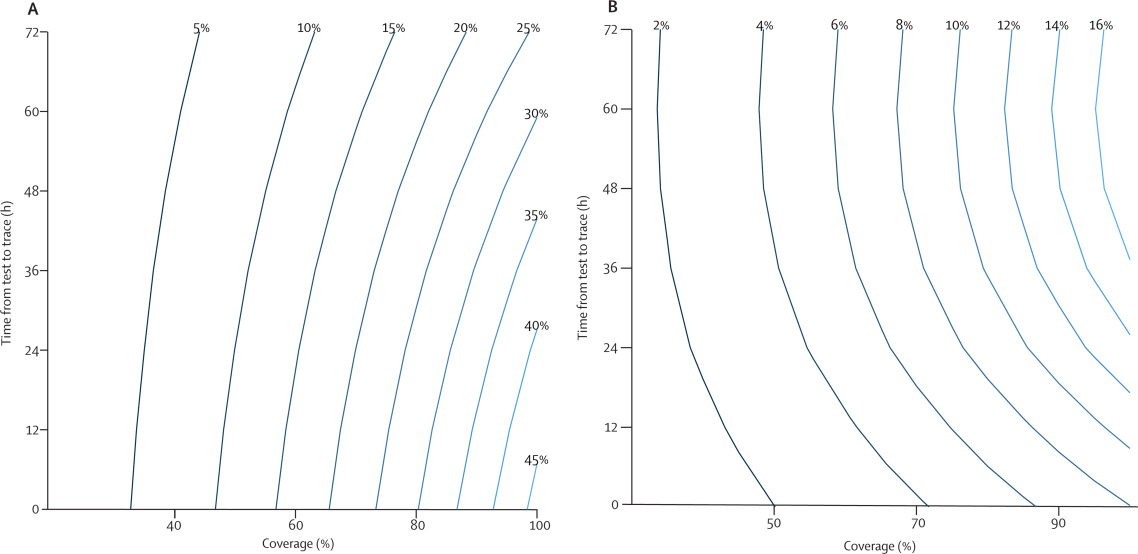
Figure 2Effectiveness of test-and-trace strategies as a function of the time from test to quarantine of contacts and coverage
Coverage is defined as the proportion of symptomatic infections identified for contact tracing and the proportion of contacts successfully traced, assumed equal in these plots. The percentage reduction in the reproduction number of contacts for test-and-trace strategies (A) or test-trace-test strategies (B), assuming self-isolation on the basis of symptoms is already in place. This reduction is approximately equal to the reduction in the overall reproduction number if contacts who develop COVID-19 symptoms are also eligible to be an index case for further contact tracing.
Contact tracing could be done on the basis of symptoms alone, rather than waiting for a test result. This approach would modestly increase the reduction in SARS-CoV-2 transmission by avoiding false-negative test results and could facilitate more rapid quarantine of contacts. For example, if all symptomatic individuals were eligible for contact tracing (equivalent to 100% test sensitivity) and the delay to quarantine was just 12 h, the reduction in transmission would increase from 26% to 31%.
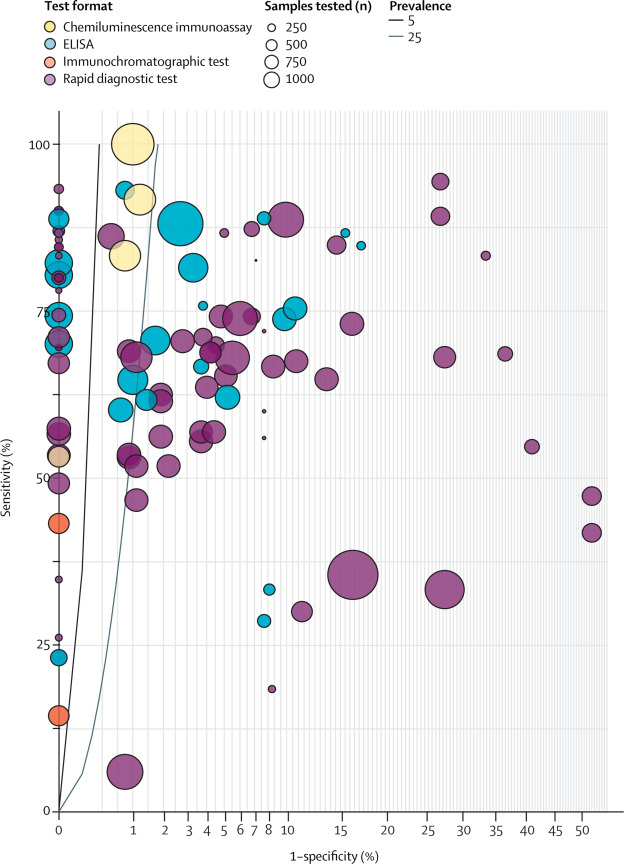
Figure 3Sensitivity and specificity of currently available antibody tests
Interactive dashboard of SARS-CoV-2 diagnostic performance data.
Discussion
- Rivett L
- Sridhar S
- Sparkes D
- et al.
,
- Shields AM
- Faustini SE
- Perez-Toledo M
- et al.
,
- Treibel TA
- Manisty C
- Burton M
- et al.
In London, UK, data from March indicated a substantially higher prevalence of 7·1% (28 of 396) in the week of March 23,
- Treibel TA
- Manisty C
- Burton M
- et al.
while seroprevalence in health-care workers in Birmingham, UK, on April 24, was 24·4% (126 of 516).
- Shields AM
- Faustini SE
- Perez-Toledo M
- et al.
It remains unclear how many of these infections were acquired from patients or from other health-care workers, although a high prevalence among staff who had no interaction with patients with COVID-19 in these studies suggests substantial transmission between health-care workers. More generally, nosocomial transmission has been an important feature of the pandemic, with UK data suggesting around 20% of patients admitted to hospital for COVID-19 acquired their infection in a hospital.
- Evans S
- Agnew E
- Vynnycky E
- Robotham JV
Tests in residential care homes done during the same period also found a high prevalence of asymptomatic infection among staff.
- Kennelly SP
- Dyer AH
- Martin R
- et al.
These and other groups with a high transmission risk and with frequent person-to-person contact, such as cashiers or teachers, might also therefore benefit from regular PCR testing during times of high SARS-CoV-2 incidence.
Detection of infected staff through regular screening or symptomatic testing also allows subsequent contact tracing at the workplace and implementation of infection control measures. Regular screening can also be complemented by mask wearing and other hygiene practices in communal areas where personal protective equipment would not typically be worn.
NHS workforce statistics — December 2019.
Weekly testing of this group would require 5000 daily tests, considerably lower than the UK target of 200 000 daily tests by the end of May, 2020. Of course, NHS staff exposed to COVID-19 include other specialties and roles, and there has been considerable reassignment of NHS staff to care for patients with COVID-19, making the number at risk who would benefit from testing difficult to determine but likely to be considerably greater than 35 000.
- Kucharski AJ
- Klepac P
- Conlan AJK
- et al.
Instead, a test-and-trace strategy based on testing of symptomatic individuals and tracing the contacts of those with laboratory-confirmed SARS-CoV-2 infection is more appropriate. However, we estimate this strategy would at best prevent about 26% (95% UI 14–35) of transmission compared with self-isolation based on symptoms alone, depending on the extent of asymptomatic transmission, assuming 80% of symptomatic infections are reported, 80% of their contacts are traced and effectively quarantined (no onwards transmission), and that testing is done on the day of symptom onset with just a 24 h delay to test results and quarantine of contacts. The combined effectiveness of self-isolation based on symptoms (47% reduction in R) and a test-and-trace strategy (26% reduction in R) would be a 61% reduction in R based on these assumptions and our best estimates of the prevalence of asymptomatic infection and its contribution to SARS-CoV-2 transmission. If R in the absence of these interventions is greater than 2·5, as estimated for most European countries at the start of the pandemic and probably still the case given the relatively low prevalence of immunity (R lower than 1.
- Flaxman S
- Mishra S
- Gandy A
- et al.
A less ambitious test-and-trace approach or one with limited compliance would have a much smaller impact on SARS-CoV-2 transmission. For example, the probability of successful contact tracing depends on the ability to identify and follow-up contacts. However, contacts at risk of infection might be difficult to identify and could include not only direct interactions but also use of shared resources or spaces within a certain time period. Compliance with quarantine measures will depend on the level of trust in the government, individual perception of risk, economic incentives and disincentives, and the ability to impose quarantine on individuals. In the case of mobile phone applications (apps) for contact tracing, their effectiveness will depend on uptake of the app and the proportion of the population with a suitable mobile phone. It is quite possible that these considerations would result in low coverage (reporting of symptoms and identification of contacts) and limited effectiveness of test and trace.
Thus, although contact tracing reduced the time to isolation of infected individuals by 1·9 days, self-isolation began on average more than a week after infection, which would lead to minimal reduction in SARS-CoV-2 transmission according to our model (corresponding to a delay from test to trace and quarantine of about 5·5 days, since without a delay we expect quarantine of contacts on average 2·5 days after infection).
- Adler AJ
- Eames KTD
- Funk S
- Edmunds WJ
Test and trace would result in fewer contacts requiring quarantine, although the number could still be substantial. For example, during the first week of test and trace implementation in England when incidence was relatively low (May 28 to June 3, 2020), 5407 (67%) of 8117 people testing positive had their contacts traced, with 26 985 contacts asked to quarantine themselves for 14 days.
Experimental statistics: weekly NHS Test and Trace bulletin, England: 28 May – 3 June 2020.
Testing of contacts and releasing those who test negative from quarantine would decrease the number in quarantine, but this approach substantially reduces the effectiveness of test and trace because of the high probability of false-negative test results in the first 3 days of infection.
- Lou B
- Li T-D
- Zheng S-F
- et al.
,
However, the effectiveness and duration of protection against subsequent exposure is unknown, particularly against heterologous strains where weak cross-neutralising antibodies could result in enhanced pathology.
- Graham RL
- Donaldson EF
- Baric RS
Finally, there are concerns that the economic and personal benefits of an immunity passport to the general population would lead to fraud, and implementation of such a scheme is likely to face serious legal and ethical challenges related to discrimination based on immune status. Perhaps, instead of an immunity passport conferring specific privileges, evidence of immunity could be used by individuals to assess their COVID-19 risk and make their own informed decisions, particularly as our understanding of immunity to SARS-CoV-2 improves and assays become more reliable. Once vaccines become available, evidence of immunity is likely to be replaced by evidence of immunisation, with most (but not all) countries unlikely to discriminate on the basis of immune status.
There are limitations to our analysis, most notably the continued uncertainty around the contribution of asymptomatic infections to SARS-CoV-2 transmission, which we have addressed through the sensitivity analysis. Data on the implementation and impact of test-and-trace strategies and on the contribution of health-care workers to nosocomial transmission are also needed. As these strategies are adopted in the UK and more widely, it is important to collect high-quality data to improve models and investigate further refinements to testing strategies.
It is clear that PCR and antibody testing are required for surveillance of the COVID-19 pandemic and will play an important role in informing the lifting or re-imposing of various components of physical distancing interventions by allowing accurate estimates of R and identifying the extent of transmission. They can also play a direct role in prevention of SARS-CoV-2 transmission, with effectiveness strongly dependent on coverage and speed to results. Now is the time to invest in testing capacity, policy, and planning to maximise their contribution to the fight against COVID-19.
Contributors
NCG conceived the study. MP-S, PJW, EPKP, and NMF provided important input on the aims of the study. NCG and MP-S developed the model. NCG coded the model and prepared the first draft of the paper. The Imperial College COVID-19 Response Team contributed to interpretation of the study results. All authors contributed to writing the manuscript and approved the final version.
Imperial College COVID-19 Response Team
Kylie Ainslie, Marc Baguelin, Samir Bhatt, Adhiratha Boonyasiri, Nick Brazeau, Lorenzo Cattarino, Helen Coupland, Zulma Cucunuba, Gina Cuomo-Dannenburg, Amy Dighe, Christl Donnelly, Sabine L van Elsland, Richard FitzJohn, Seth Flaxman, Keith Fraser, Katy Gaythorpe, Will Green, Arran Hamlet, Wes Hinsley, Natsuko Imai, Edward Knock, Daniel Laydon, Thomas Mellan, Swapnil Mishra, Gemma Nedjati-Gilani, Pierre Nouvellet, Lucy Okell, Manon Ragonnet-Cronin, Hayley A Thompson, H Juliette T Unwin, Michaela Vollmer, Erik Volz, Caroline Walters, Yuanrong Wang, Oliver J Watson, Charles Whittaker, Lilith Whittles, Xiaoyue Xi.
Declaration of interests
We declare no competing interests.
Acknowledgments
We thank Ruth McCabe and Alessandra Lochen in the Imperial College COVID-19 hospitalisation and economics team for helpful discussions about NHS staffing. We acknowledge funding from the MRC Centre for Global Infectious Disease Analysis (MR/R015600/1); this award is jointly funded by the UK Medical Research Council (MRC) and the UK Department for International Development (DFID) under the MRC/DFID Concordat agreement and is also part of the EDCTP2 programme supported by the European Union.
Supplementary Material
References
- 1.
Dynamic CO-CIN report to SAGE and NERVTAG.
- 2.
Informe sobre la situación de COVID-19 en España. Informe COVID-19 no 22.
- 3.
Coronavirus (COVID-19) infection survey pilot.
- 4.
The impact of testing and infection prevention and control strategies on within-hospital transmission dynamics of COVID-19 in English hospitals.
medRxiv. 2020; ()
- 5.
Time is of the essence: impact of delays on effectiveness of contact tracing for COVID-19.
medRxiv. 2020; ()
- 6.
Effectiveness of isolation, testing, contact tracing, and physical distancing on reducing transmission of SARS-CoV-2 in different settings: a mathematical modelling study.
Lancet Infect Dis. 2020; ()
- 7.
Periodic COVID-19 testing in emergency department staff.
medRxiv. 2020; ()
- 8.
Mathematical models of infectious disease transmission.
Nat Rev Microbiol. 2008; 6: 477-487
- 9.
Quantifying antibody kinetics and RNA shedding during early-phase SARS-CoV-2 infection.
medRxiv. 2020; ()
- 10.
Variation in false-negative rate of reverse transcriptase polymerase chain reaction-based SARS-CoV-2 tests by time since exposure.
Ann Intern Med. 2020; ()
- 11.
Estimating false-negative detection rate of SARS-CoV-2 by RT-PCR.
medRxiv. 2020; ()
- 12.
Interactive dashboard of SARS-CoV-2 diagnostic performance data.
- 13.
Screening of healthcare workers for SARS-CoV-2 highlights the role of asymptomatic carriage in COVID-19 transmission.
eLife. 2020; 9e58728
- 14.
SARS-CoV-2 seroconversion in health care workers.
medRxiv. 2020; ()
- 15.
COVID-19: PCR screening of asymptomatic health-care workers at London hospital.
Lancet. 2020; 395: 1608-1610
- 16.
Asymptomatic carriage rates and case-fatality of SARS-CoV-2 infection in residents and staff in Irish nursing homes.
medRxiv. 2020; ()
- 17.
NHS workforce statistics — December 2019.
- 18.
Estimating the effects of non-pharmaceutical interventions on COVID-19 in Europe.
Nature. 2020; ()
- 19.
Epidemiology and transmission of COVID-19 in 391 cases and 1286 of their close contacts in Shenzhen, China: a retrospective cohort study.
Lancet Infect Dis. 2020; 20: 911-919
- 20.
Incidence and risk factors for influenza-like-illness in the UK: online surveillance using Flusurvey.
BMC Infect Dis. 2014; 14: 8
- 21.
Experimental statistics: weekly NHS Test and Trace bulletin, England: 28 May – 3 June 2020.
- 22.
Neutralizing antibody responses to SARS-CoV-2 in a COVID-19 recovered patient cohort and their implications.
medRxiv. 2020; ()
- 23.
Serology characteristics of SARS-CoV-2 infection since exposure and post symptom onset.
Eur Resp J. 2020; ()
- 24.
Effectiveness of convalescent plasma therapy in severe COVID-19 patients.
Proc Natl Acad Sci USA. 2020; 117: 9490-9496
- 25.
A decade after SARS: strategies for controlling emerging coronaviruses.
Nat Rev Microbiol. 2013; 11: 836-848
Article Info
Publication History
Published: August 18, 2020
Identification
Copyright
© 2020 The Author(s). Published by Elsevier Ltd.
User License
ScienceDirect

Cory Weinberg is a contributor to Sproutwired.com, covering a wide range of topics including news, politics, business, technology, sport, entertainment and lifestyle. He focuses on delivering clear, balanced reporting that helps readers stay informed about current events and emerging developments. Cory’s work highlights relevant stories, practical insights and important issues affecting communities and industries, with an emphasis on accuracy, clarity and information that readers can trust.


